

Atrial Fibrillation (AF) is the most common heart rhythm disorder, characterised by an irregular heart rate that is no longer driven by the body’s usual pacemaker the sinoatrial node. Instead, by a chaotic and rapid electrical activation of the atria, known as the upper chambers of the heart. A loss of mechanical contraction of the atria, and synchronisation of the atria and the ventricles, lower chambers of the heart, results in a rapid and irregular heart rate and a reduction in the efficiency of the heart function. Blood flow is also impaired, leading to an increased risk of clot formation, giving rise to a higher possibility of stroke.
Often, there is no single reversible cause of AF. It may be associated with several conditions and triggered by many factors. In general, AF is associated with aging. It is rare in people under 40 years old and can be present in up to 15% for people over 80 years old.
Other conditions that might cause AF may include:
People with AF may be either asymptomatic, with no overt symptoms; or could have serious or even life-threatening symptoms of stroke, a focal neurological deficit such as weakness, loss of sensation or loss of speech, or heart failure – breathlessness due to water in the lungs and/or swelling of the legs due to water retention.
The most common symptoms of AF are:
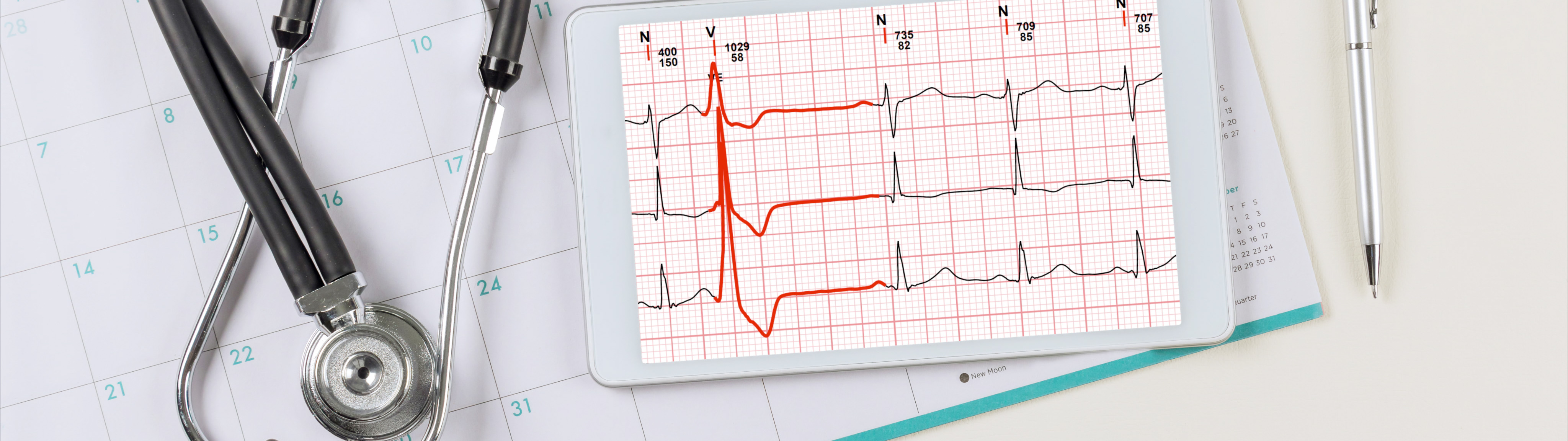
AF is diagnosed by a 12-lead electrocardiogram (ECG) or by a single or multi-lead ECG monitoring. Increasingly, smartwatches with ECG recording capabilities and algorithms that analyse heart rhythm may also aid in the diagnosis of AF. Upon confirmation of AF via an ECG, the doctor may request for other tests such as a blood test to check thyroid function, or on salt levels, i.e., potassium, calcium, etc.
Once diagnosed with AF, it is important to have regular follow up. For those on strong medications to control their heart rhythm, it is often necessary to monitor their ECG and go for frequent blood tests. For those on anti-coagulants, it is important to monitor their haemoglobin count, kidney function and heart function to look out for any development of heart failure symptoms over time.
The overall management of AF can be simplified into “ABC” as recommended by the European Society of Cardiology.
AF results in a loss of atria contraction, leading to blood stasis and risk of blood clot formation, giving rise to an increased risk of stroke.
The most accepted way to reduce stroke risk is to take medications, anti-coagulants, to “thin” the blood. However in some patients, a procedure to close off the left atrial appendage, a cardiac structure where most of the blood clots form, may be considered, especially if anti-coagulants are contra-indicated or poorly tolerated by patients.
In general, symptoms of AF stem from the fast heartbeats and/or the loss of synchrony between the atria and ventricles. Medications (e.g., beta-blockers and calcium channel blockers) are prescribed to control heart rate or restore and maintain normal heart rhythm. However, some medication may not be effective in controlling the heart rhythm and may cause side effects.
Catheter ablation can be considered for a more definitive and effective way to control the heart rhythm. This is a minimally invasive procedure to eliminate the electrical signals that trigger AF. In a few cases, implantation of a pacemaker may be necessary to help regulate the heart rate.
Pacemaker
A pacemaker is a device implanted underneath the skin in the chest that sends small electrical impulses to the heart muscle to maintain a suitable heart rate or stimulate the ventricles.
The pacemaker consists of two parts: a box that houses the electronics (the “device”) and one or more wires that connect the box to the heart muscle (the “leads”). The doctor will determine the minimum heart rate to set for the pacemaker and when the patient’s heart drops below the set rate, it will generate an impulse that passes through the lead to the heart muscle. This causes the heart muscle to contract, creating a heartbeat.
As AF is commonly associated with certain cardiovascular risk factors (e.g., high blood pressure, diabetes, obesity, sedentary lifestyle, etc.) and other comorbidities (e.g., obstructive sleep apnoea). Lifestyle modifications such as regular exercise and diet changes can help to achieve weight loss and improve cardiovascular fitness, which have shown to improve symptoms of AF.
Treatment such as non-invasive continuous positive airway pressure ventilation (CPAP) can also be used to treat obstructive sleep apnea, which has shown to improve outcomes of AF.
Continuous Positive Airway Pressure Ventilation
CPAP is a type of positive airway pressure that is used to deliver a set pressure to the airways that is maintained throughout the respiratory cycle, during both inspiration and expiration. It is a simple concept with three basic parts: an air pump (CPAP machine), a mask that covers the nose and sometimes the mouth and a tube that connects both items together.
It is usually used at night or during sleep, to prevent breathing difficulties, increase the level of oxygen in the lungs and remove carbon dioxide from the lungs. It helps reduce disruption to sleep, improve sleep quality and improve daytime functioning.
In general, AF tends to be a progressive and chronic condition. Hence, in most cases, people must live and cope with AF just like many other chronic conditions such as high blood pressure, high blood cholesterol and diabetes. However, there are cases where AF may be treated successfully. This is usually in younger patients who have undergone successful catheter ablation.
In many cases, people can lead an unrestricted lifestyle if the AF is well controlled. Restrictions would need to be tailored. People with AF have to understand their possible triggers. Gastric issues may be a trigger for AF in some people, hence it would be important to avoid certain food and drinks which may exacerbate their gastric issues.
Getting AF is not a death sentence. There are ways to control it and improve your quality of life. Treatment of AF is as easy as ABC! See your doctor, take your medication and maintain a healthy lifestyle.